I started this blog as a requirement for a graduate course taught by www.twitter.com/drbret while I was enrolled at University of Nevada Reno’s Executive Master of Business Administration (MBA) www.twitter.com/embaunr program from August 2020 – August 2022. This course in particular has been very fulfilling for me in many ways. As was the complement of the course curriculum, and succeeding in my personal growth. To be enrolled and to earn an MBA degree to further advance my career leadership skills.
I was able to be introduced to and to learn about several forms of online marketing through additional website development, social media sites I joined, and profiles that I produced to showcase my: personal story, life path, career experiences, and a connected professional brand that I selected to explore marketing to the public.
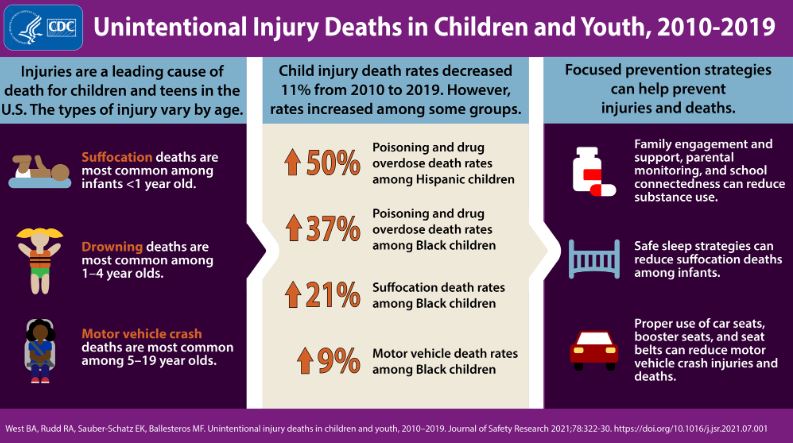
As you may know, my brand has focused on preventing injuries by consulting with communities to identify their biggest injury challenges and helping communities to select strategies and launch action plans through community engagement and capacity development. Using advocacy, awareness, buy-in & collaboration with private business, non-profits, faith-based & public sectors of the local community entities. Making it possible to strategically expand the reach of prevention strategies, through education, environment changes, enforcement changes, engineering & re-development of lands & buildings. In order to eliminate risk factors and to generate protective factors leading to a more resilient & higher quality of life community over time.
For example, creating single story, Americans with Disabilities Act (ADA) adapted design, and cost adjusted, to fixed income rental rates, housing options for seniors, with on-site exercise studio & physical therapy supported services. With the focus to assist senior tenants to prevent falls & extend their quality of life over their final 12 – 18 years. While the residents of this housing option would avoid falls injuries and hospitalizations. Which can be followed by costly intensive medical services recovery and result in earlier moves to assisted living care. With life expectancy shortened by 5 – 7 years, and earlier deaths.
Without this approach there is the risky alternative, possibly falls down stairs, a feature mismatched from being an ideal living environment for seniors. Or falls in the bathroom due to the lack of ADA grab bars or ADA toilet height riser attachment. Of a fall at the building entry also not adapted with a ramp, and having stairs that become difficult to maneuver as seniors age. All these risks, a challenge for seniors created simply from remaining in their long term residence, which lacks design change or adaptation for the purpose of aging in place. Because otherwise, without community planning, and advocacy, no better option may be available or studied or planned or designed to be available to allocate and link the resources to this vulnerable subset of the community population at risk of costly injuries.
See this is the purpose of what I learned in building a brand. Your presence on a website, on social media, with constant added and updated content perspectives that draw from the latest news, research, science advancement, peer reviewed articles and even results from legislative actions and government agency actions, are on display day and night and in all places where the internet exists 24/7. This is a powerful way to be discovered, to be known for your brand, and for your brand to be leading the kinds of ideas that create the changes you want to see. It also allows for continued improvement, for personal growth through knowledge attainment and continued lifelong learning by way of research. To develop content and share ideas with the public in a dialogue filtered through the social media site.
You know we talked about the invisible hand and how a brand developer does what is in their best interest, yet in many ways the social contract we adhere to by publicly posting our brand upholds ethical information sharing and value to others in the authenticity and emotional impact of the brand. The changes will also come from this positive energy and dialogue with the public and the followers of an online brand. The honesty & integrity are critical, avoiding misinformation a form of half truths and at times outright lies will be the only way to serve a brand’s purpose to invite the public to trust and share in the brand’s value.
This has been a great journey for me. I plan to continue to add content to this site to keep my brand going and expanding my reach as more people discover this website, my twitter account: www.twitter.com/Martin_NV_GA_AZ , or my LinkedIn account: https://www.linkedin.com/in/martin-stephens-ph-practice/ Thank you for visiting and reading my blog.